
.png)

There's a structure in the middle of your nose so fundamental to breathing that its absence — or its misalignment — can quietly unravel your sleep, your energy, and your ability to tolerate a CPAP machine. Most people have never heard of it. Some have been told they have a deviated one and promptly forgot about it. A few have been living with its consequences for decades without realizing the source.
We're talking about the nasal septum.
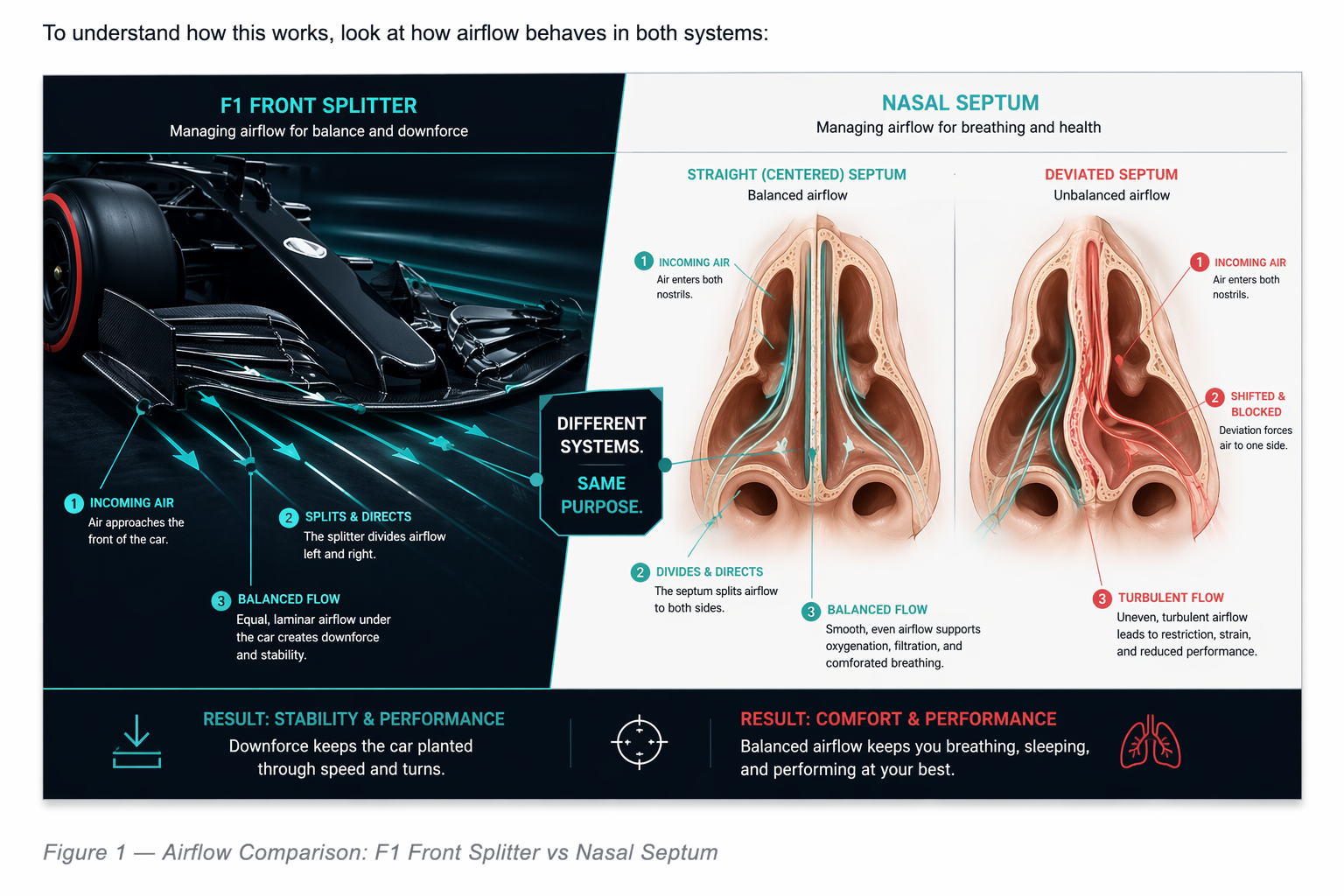
In Formula 1, there's a component at the very front of the car called the front splitter. It's a horizontal blade that slices incoming air and directs it with equal precision to both sides of the underfloor — creating balanced aerodynamic load, laminar flow, and maximum downforce. When it's intact and centered, the car is planted, stable, and fast. When it's cracked, bent, or asymmetric, the whole aerodynamic platform destabilizes. Downforce drops on one side. The driver fights the car instead of racing it.
Your nasal septum is that front splitter.
This issue, we take it apart — how it's built, how it fails, what it costs you when it does, and what it looks like when you finally get it right.
🔧 TECH SPEC BRIEFING
The Engineering Behind the Anatomy
Built to Divide and Conquer
The nasal septum is the central wall of the nose — a thin but precisely engineered partition that runs from the base of your nostrils all the way to the back of your nasal cavity, dividing it into a left channel and a right channel. It's made of two materials working in tandem: cartilage in the front (the quadrangular cartilage), which is flexible and acts as a shock absorber; and bone in the back (the perpendicular plate of the ethmoid and the vomer), which forms a rigid keel that anchors and stabilizes the entire midline structure.
Together, these segments are just a few millimeters thick — yet they define whether air flows symmetrically and smoothly through both nasal passages, or turbulently and unevenly through one.
When the septum is straight, air enters both sides in equal, balanced streams. Pressure is distributed evenly. Airflow is laminar. The system runs efficiently — just like an F1 car with a perfectly centered front splitter generating equal downforce on both sides.
When the septum deviates — shifting to one side through a bend, buckle, or twist — the intake becomes asymmetric. One channel narrows. Airflow accelerates and becomes turbulent through the tight side. The wider side compensates unevenly. The whole system loses efficiency, and the body starts making trade-offs it was never meant to make.
Why Deviations Happen
Septal deviations are extraordinarily common — present in close to 70% of the population in some form. Most cause no meaningful symptoms. But a significant number do, and understanding why the septum deviates in the first place helps explain why it's so prevalent.
There are three main mechanisms:
- Genetics — the shape and position of septal cartilage has a hereditary component. Some families simply pass down a predisposition toward deviation.
- Birth — as the head travels through the birth canal, compressive forces can torque the facial skeleton and displace the septum before a person even takes their first breath.
- Trauma — a blow to the nose, whether from a fall, a sport, or an accident, can fracture or displace the septum. These traumatic deviations tend to occur in the anterior (front) segment, where they're most likely to obstruct airflow.
The Physics of a Bent Splitter
When air encounters a deviated septum, the physics of the situation work against you in a very specific way. On the narrowed side, airflow velocity increases — which, per Bernoulli's principle, drops local pressure and promotes turbulence rather than smooth laminar flow. Resistance across the entire nasal passage rises. Your diaphragm and chest muscles have to work harder with every single breath.
Over time, the body adapts — and not well. It shifts to mouth breathing. Snoring increases as upper airway tissues collapse. Sleep becomes fragmented as the airway struggles to maintain adequate flow during the relaxed state of sleep. And for patients who use CPAP for sleep apnea, a deviated septum can make the mask nearly impossible to tolerate — not because the pressure settings are wrong, but because the intake itself is misaligned.
In performance terms: it's like trying to race with a bent front splitter and asymmetric tire pressures. The car still moves. But it will never be fast.
⚙️ THE ENGINEERING INSIGHT
Even a 2–3mm deviation inside the nasal septum can cause a dramatic rise in nasal resistance — enough to alter sleep architecture, fragment deep sleep cycles, and reduce oxygen exchange efficiency. In F1, a 2–3% loss in laminar airflow can cost seconds per lap. The same physics, the same consequences.
Small misalignment. Large performance cost.
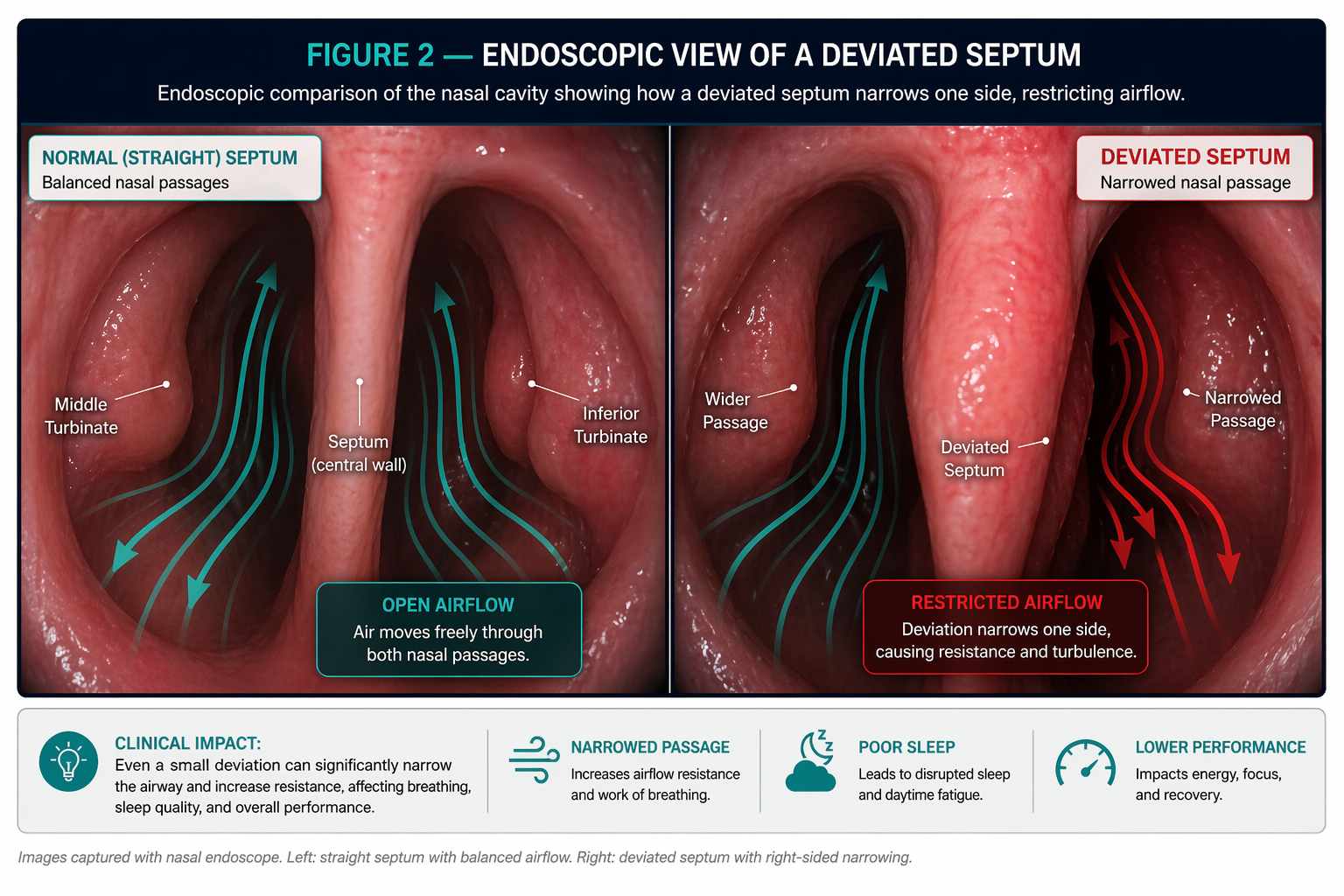
Diagnosing the Deviation: How We Map It
ENT surgeons evaluate the septum both visually and functionally. A nasal endoscope — a thin, lighted camera — lets us look directly inside the nasal cavity and map the deviation's location and pattern:
- A C-shaped deviation bends primarily to one side, obstructing one nasal channel.
- An S-shaped deviation twists in both directions — narrowing both sides at different levels.
- A high dorsal deflection sits near the nasal valve, where even a small deviation causes significant obstruction because the valve is already the narrowest point in the airway.
When the clinical picture is complex or surgery is being planned, a CT scan gives us a three-dimensional map of the deviation — showing where the bone and cartilage are displaced, how they relate to the turbinates, and whether the sinuses are involved.
The Fix: Septoplasty
When medical therapy — nasal steroid sprays, antihistamines, decongestants — fails to restore adequate airflow, the next step is surgical correction: a septoplasty.
Septoplasty is a precise, targeted procedure aimed at one goal: straightening the septum to restore laminar, balanced airflow. Here's what it actually involves:
- All incisions are made inside the nose — no external cuts, no visible scars, no change to the outside appearance of your nose.
- The mucosa (the soft lining of the septum) is carefully elevated on both sides, like lifting the bread of a sandwich off the filling.
- The deviated cartilage and bone are reshaped or removed, while the structural support of the nose is preserved.
- The lining is placed back down and sutured.
- Modern technique uses soft internal splints or sutures — not the uncomfortable gauze packing that many patients fear from older descriptions of the surgery.
The procedure takes about an hour under general anesthesia. Patients go home the same day.
RECOVERY TIMELINE
WHAT TO EXPECT
Night 1
Feels like a bad head cold — stuffy and congested. This is normal swelling from the surgery.
Days 2–4
Gradual improvement. Little to no pain for most patients. Your surgeon will see you to clear any crusting.
Day 4–5
Most patients return to work, driving, and daily routines.
Week 2
Breathing begins to noticeably improve as swelling resolves. Do not blow your nose.
Week 3
Cleared for light exercise. Nasal saline irrigation starts in week 1–2.
Week 4
Full breathing benefit typically realized. Most patients report feeling significantly clearer than before surgery.
📐 SEPTOPLASTY vs. RHINOPLASTY — KNOW THE DIFFERENCE
Septoplasty repairs the inside of the nose. It improves airflow, reduces obstruction, and addresses functional breathing problems. Insurance typically covers it when medically indicated.
Rhinoplasty reshapes the outside of the nose. It adjusts nasal bones, cartilage, and external appearance. It is considered cosmetic and is not covered by insurance.
These are two separate operations — even though they can be performed together when both functional and cosmetic goals exist. If you're considering both, speak to your ENT and a facial plastic surgeon before proceeding, as the order matters for preserving available cartilage.
🏎️ PADDOCK PASS
A Story from Inside the Garage
Sergio's Story: The Machine Wasn't the Problem
Sergio had been on CPAP for two years when he came to see me.
He wasn't a new patient to the sleep system — he'd been through the study, the diagnosis, the mask fittings, the pressure titrations. His sleep doctor had tried three different masks. His compliance data showed he was using the machine, but only for two to three hours before he pulled it off in frustration. He woke exhausted. His wife still elbowed him for snoring — with the mask on.
Everyone assumed the CPAP wasn't working because of the apnea severity, or the mask interface, or his sleep position. Nobody had looked inside his nose.
"I've never actually seen an ENT," he told me. "My sleep doctor said to try a different mask."
When I looked inside with the endoscope, what I found was a significant C-shaped septal deviation — the septum pushed hard to the left, leaving a narrow corridor where the right side should have been open and flowing. The CPAP pressure was fighting the deviation every single night. The machine was trying to hold the airway open against a structural wall.
We talked about his options. Medical therapy wasn't going to move cartilage. A septoplasty was the right call.
Six weeks after surgery, Sergio came back for his follow-up. He'd been on CPAP for the full night — every night — for the first time since he was diagnosed. His compliance data looked like a different patient. "The machine feels like nothing now," he said. "I don't even notice it."
The CPAP hadn't changed. The pressure settings hadn't changed. The only thing that changed was the splitter — finally straight, finally balanced, finally letting air move the way it was supposed to.
That's the part that often gets missed: optimizing sleep apnea treatment isn't always about the therapy device. Sometimes it's about the intake system the device depends on.
⚡ DRS ENABLED
One Actionable Win You Can Use Today
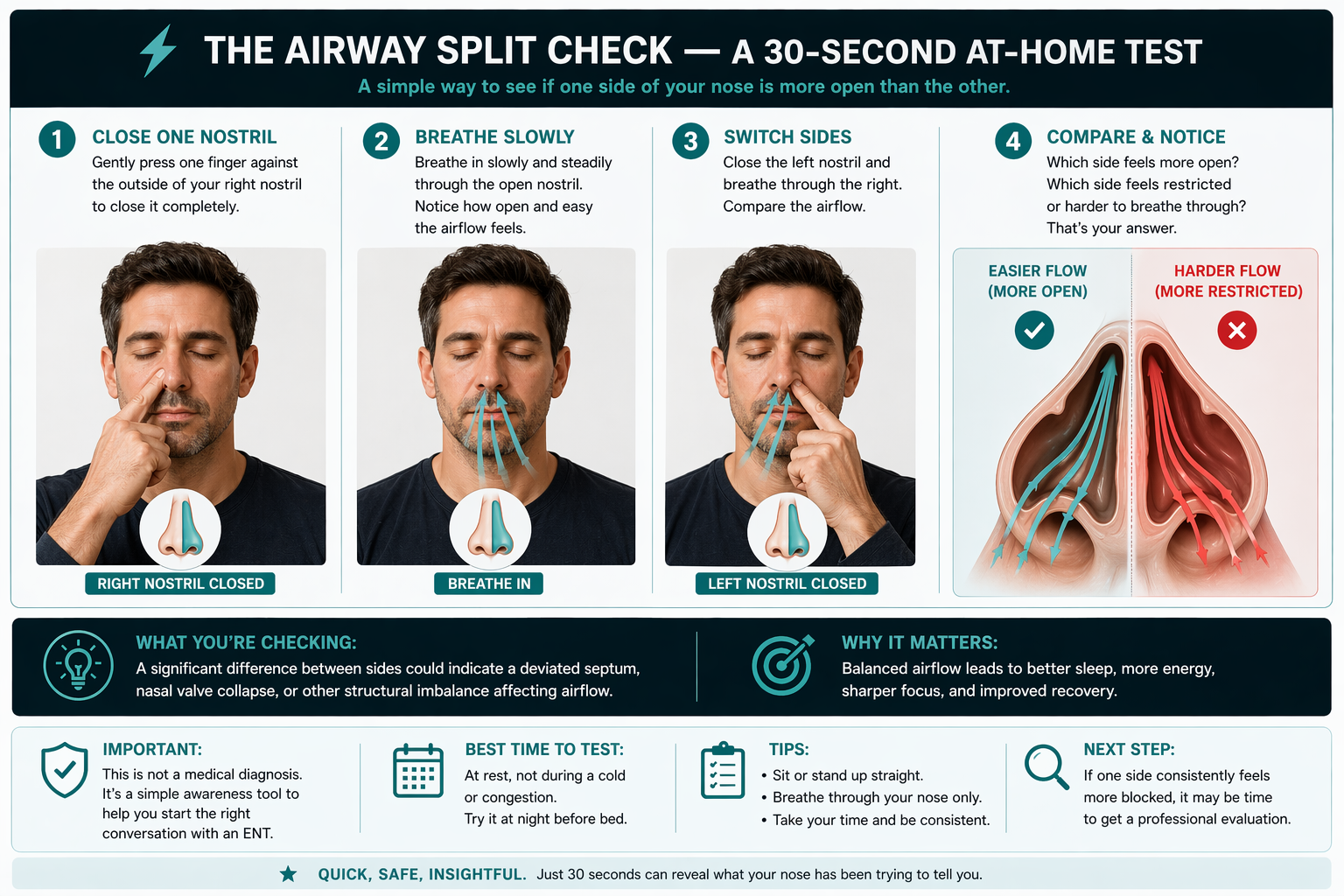
⚡ THE AIRWAY SPLIT CHECK — A 30-Second At-Home Test
Here's a simple diagnostic you can run right now — no equipment, no appointment:
Step 1: Gently press one finger against the outside of your right nostril to close it completely.
Step 2: Breathe in slowly and steadily through the left nostril. Notice how open and easy the airflow feels.
Step 3: Switch sides. Close the left nostril and breathe through the right. Compare.
What you're checking: Is one side dramatically harder to breathe through than the other? Do you feel like you're always defaulting to mouth breathing on one particular side at night? Is there a persistent sense of blockage that doesn't shift — that isn't affected by blowing your nose or using a saline spray?
A significant, consistent difference between sides is a signal worth paying attention to. It doesn't tell you exactly what's happening — the turbinates, the nasal valve, and the septum all live close together and can overlap in their effects. But if one side is always the restricted one, and medical therapy hasn't solved it, the splitter may be off-center.
This isn't a diagnosis. It's a starting point for a real conversation with your ENT.
📋 TECHNICAL REGULATIONS
This Issue's Safety Check
📋 WHAT A SEPTOPLASTY WILL — AND WON'T — DO FOR YOU
One of the most common conversations I have after recommending a septoplasty goes like this: "If I fix my septum, will I be able to get off CPAP?" It's a reasonable question. Here's the honest answer.
What septoplasty WILL do:
- Restore balanced, laminar airflow through both nasal passages.
- Dramatically improve CPAP comfort and compliance — patients who struggled with 2–3 hours often achieve full-night use after surgery.
- Reduce the pressure settings required for effective CPAP in many patients.
- Improve sleep quality, reduce snoring, and reduce mouth breathing — if those symptoms were primarily driven by nasal obstruction.
- Allow allergies and nasal inflammation to be treated more effectively — an open airway responds better to sprays and rinses.
What septoplasty WILL NOT do:
- Cure obstructive sleep apnea. Fixing the intake improves the system but is only one section of the airway which results in sleep apnea.
- Treat allergies or chronic sinusitis. Those are separate conditions requiring separate management.
- Change the external appearance of your nose. A septoplasty operates entirely inside the nose — no bruising, no cast, no cosmetic alteration.
The technical regulation: treat the septum as one component in a larger system. When it's the limiting factor, fixing it unlocks everything downstream. But it's rarely the only component that needs attention — which is exactly why a thorough ENT evaluation matters before surgery.
Balancing the Intake
The septum doesn't get the attention it deserves. It doesn't cause dramatic visible symptoms. It doesn't show up on a blood panel or in a routine physical. It quietly taxes every breath you take — and over a lifetime, those taxes compound.
But when you realign the splitter? The whole system comes back into balance. Air flows where it's supposed to flow. The body stops compensating. Sleep gets deeper. CPAP becomes tolerable. The fatigue that you assumed was just how you are turns out to be a structural problem with a structural solution.
That's what Aerodynamic Medicine is built on: finding the specific component that's limiting the system, and engineering the fix.
The septum is Issue 4's component. And for a lot of people, it's the one nobody ever checked.
The ENT Edge
Join Dr Gus on Substack for more actionable wellness insights and guides to help you sleep, breathe, and hear better, with spotlights on new technologies in the ear, nose and throat health category.

.jpg)