
.png)
.jpg)
OPENING — KRISTINA'S STORY
Kristina was 42 years old and she was nervous before I even said hello.
I could tell the moment she sat down in my exam chair. Arms crossed, quiet. The kind of stillness that isn't calm — it's bracing. After a few minutes I asked her directly: "What's worrying you today?"
She hesitated, then said it.
"I'm scared it's a tumor. Or a polyp. Something growing in my nose."
She told me she'd been congested for years — the kind of congestion that never really clears, no matter the season, no matter how many sprays she tried. A few weeks earlier, she'd looked up her symptoms online. A mistake, as it often is. She'd read about nasal tumors. Convinced herself that's what this was.
When I scoped her — passed a small camera gently through her nose — I could immediately see what was happening. The view down her nasal passage was almost completely blocked. But it wasn't a tumor. It wasn't a polyp. It was something far more common and far more treatable.
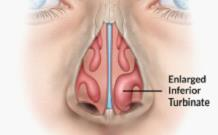
Her inferior turbinates were so swollen from years of untreated allergic inflammation that they'd filled the nasal cavity. Chronic allergic rhinitis had turned her internal "ductwork" into something that looked, on camera, like a mass.
This is more common than you'd think. A severely inflamed inferior turbinate, viewed head-on through a nasal scope, can genuinely mimic the appearance of a polyp or growth. It's a visual that sends patients into panic. And it's one of the most important things I explain in my practice: what you're seeing is not a tumor — it's your airway choking on chronic inflammation.
Kristina left my office that afternoon with a clear diagnosis, a treatment plan, and — most importantly — the explanation she needed. The fear disappeared the moment she understood what was actually happening inside her nose.
That's what this article is about.
🔧 TECH SPEC BRIEFING — THE ENGINEERING BEHIND THE ANATOMY
The F1 Air Intake Analogy: Meet Your Turbinates
If we established in Issue 2 that the nasal valve is your airway's front wing — the narrowest, most structurally critical point — then this issue we're going one step deeper, into the interior of the duct itself.
Inside each side of your nose, running from front to back, are three long curved structures called turbinates — the superior, middle, and inferior. Their formal name sounds mechanical because, in every meaningful sense, they are mechanical.
🔧 TECH SPEC
Think of your turbinates as the aerodynamic fins lining the inside of a high-performance air intake duct.
In Formula 1, the intake system doesn't just funnel raw air into the engine — it conditions that air. Every curve and duct is engineered to warm the air, filter particulates, manage humidity, and smooth out turbulence before the air reaches the combustion chamber. The goal is laminar flow: clean, smooth, pressurized air moving efficiently through the system.
Your turbinates do exactly the same thing. Every breath you take — all 20,000 of them per day — passes over these scroll-shaped structures. They warm incoming air to body temperature, filter bacteria and particles, add moisture so your lungs don't dry out, and shape the airstream to reduce turbulence. They are the intercooler, the particle filter, and the flow conditioner of your nasal engine, all in one piece of living tissue.
The Inferior Turbinate: Your Variable Intake Valve
Of the three turbinates, the inferior turbinate is the one that matters most to most people — and the one most likely to be causing your symptoms.
It's the largest and the lowest of the three structures. And here's the key: it's not static. Unlike the cartilage of the nasal valve or the bony walls of the sinus, the inferior turbinate is covered in highly vascular, dynamic mucosa — living tissue packed with blood vessels that can swell or shrink on command.
Think of it like a variable geometry intake — a system found in some high-performance engines that adjusts the shape of the intake duct in real time depending on engine load. At lower RPMs, the duct narrows to maintain velocity. At high RPMs, it opens up to flow more volume. Your inferior turbinate does something similar. It swells when your body needs more humidification and filtration; it shrinks when it needs to let more air through.
This is also why you may notice that one nostril always seems more blocked than the other — and that it switches sides periodically. That's not congestion. That's the nasal cycle: a normal physiological rhythm where your body alternates which turbinate is slightly expanded, roughly every 2–4 hours. Both sides are open; one is just doing more conditioning work than the other at any given moment.
💡 THE NASAL CYCLE — A NORMAL PHENOMENON MOST PEOPLE DON'T KNOW EXISTS
If you've ever noticed that one nostril is more open in the morning and the other takes over by afternoon — that's your body's nasal cycle at work, not congestion.
It's a normal, regulated process. Your autonomic nervous system deliberately alternates congestion between left and right turbinates every 2–4 hours. The total airflow stays consistent; only the distribution shifts.
It becomes a problem when both sides are chronically swollen — which is what allergic rhinitis does. Then the cycle doesn't just redistribute airflow. It oscillates between 'barely open' and 'almost closed.'
When the Duct Gets Clogged: Turbinate Hypertrophy
Turbinate hypertrophy simply means the inferior turbinate has become persistently enlarged — not temporarily, as in the nasal cycle, but chronically. The duct is partially blocked all the time.
In engineering terms, it's the equivalent of a foreign object caught in the intake duct, or a buildup of debris narrowing the passage over time. Air still flows — but it flows turbulently, inefficiently, against resistance.
And here's where the physics from Issue 2 comes back. You'll remember Poiseuille's Law — the principle that airflow through a tube is proportional to the fourth power of the radius. A small reduction in the diameter of the nasal airway doesn't create a proportionally small reduction in airflow. It creates a massive, exponential reduction. A turbinate that occupies even a modest portion of the nasal cavity can cut airflow dramatically.
🔧 WHAT TURBINATE HYPERTROPHY DOES TO YOUR BODY
• Nasal obstruction — persistent stuffiness that decongestants only partially relieve
• Sleep disruption — mouth breathing, snoring, fragmented sleep, and reduced deep sleep
• Reduced oxygen efficiency — turbulent airflow means less laminar, efficient oxygen exchange
• Increased breathing effort — your body works harder to pull air past the obstruction, especially lying flat
• Downstream effects — chronic mouth breathing can alter jaw development in children, cause dental issues, and dry out the throat and airway
Why Does the Turbinate Enlarge?
There are several common culprits, and understanding which one is driving your symptoms is the first step toward the right fix.
Allergic Rhinitis
By far the most common cause. Chronic exposure to allergens — dust mites, pollen, pet dander, mold — triggers ongoing immune-mediated inflammation in the nasal lining. The turbinate tissue swells as part of that immune response, and because the exposure is continuous, the swelling becomes continuous. This is exactly what was happening to Kristina.
Medication Rebound — The Afrin Trap
I covered this briefly in Issue 1, and I'll reinforce it here because I see it constantly. Oxymetazoline (Afrin) and similar topical decongestants provide real, fast relief. They also create dependency. Use them for more than 3 days consecutively, and your turbinate tissue becomes dependent on the medication to stay contracted. When the spray wears off, the tissue swells even more than before. This is called rhinitis medicamentosa — rebound congestion — and it can be worse than whatever you started treating.
Structural Variation and Compensatory Hypertrophy
When the nasal septum deviates significantly to one side, the opposite nasal passage often becomes relatively too open. The inferior turbinate on that side will naturally enlarge to compensate — a biological effort to maintain resistance and keep airflow conditioning working. It's adaptive physiology that ends up creating an obstruction on the 'good' side.
Environmental and Hormonal Triggers
Dry air, pollution, hormonal fluctuations (pregnancy is a classic example — many women experience significant nasal congestion), hypothyroidism, and certain medications (including some blood pressure drugs) can all cause turbinate swelling. The turbinate is a sensitive structure; it responds to the environment it lives in.
🏎️ PADDOCK PASS — BST CORNER
The Scope That Changed Everything
I want to come back to Kristina for a moment — not because her case was unusual, but because of what she said after I showed her the scope images.
After I walked her through what the camera showed — the swollen turbinates, the narrowed airway, why it looked the way it did — she was quiet for a moment. Then:
“I’ve never seen an ear, nose, and throat doctor before. Now I finally understand what’s been going on.”
That kind of moment happens regularly in ENT practice, and it’s one of the things I value most about what we get to do. A nasal endoscopy is a simple, in-office procedure — a thin, flexible camera passed gently through the nose. It takes a few minutes. It’s well-tolerated. And it gives both the physician and the patient a direct view of anatomy that simply cannot be assessed from the outside.
For chronic nasal congestion, snoring, recurring sinus infections, or unexplained nasal symptoms, a scope changes everything. It’s the difference between treating a symptom and understanding a system. In Kristina’s case, it was the difference between fear and clarity — in a single appointment.
If you have been living with nasal symptoms that haven’t been fully explained, it may simply be that you haven’t had the opportunity to see what’s actually happening inside. That’s what this newsletter is here to help with — and when words and images aren’t enough, that’s what an ENT visit is for.

HOW WE DIAGNOSE — AND FIX — THE PROBLEM
Diagnosis: It Starts With a Scope
Turbinate hypertrophy is a clinical diagnosis — meaning we can identify it by examining the nose directly. A flexible nasal endoscope (a thin, lighted camera) gives a clear view of the turbinate size, the degree of obstruction, and whether other structures are involved.
In the office, I also look at the full nasal anatomy: the septum, the nasal valve, the middle turbinate and the sinus openings. Turbinate hypertrophy rarely exists in isolation. It often coexists with a deviated septum (which we'll cover in Issue 4) or chronic sinusitis. Understanding the full picture is what allows us to design the right treatment plan.
Treatment: From Sprays to Procedures
Treatment follows a logical progression — least invasive first, escalating based on response.
Step 1: Address the Inflammatory Trigger
If allergic rhinitis is driving the hypertrophy — which it is in the majority of cases — the first priority is calming the immune response. This means a combination of:
- Topical nasal steroid sprays (Flonase, Nasacort) — reduce mucosal inflammation over time
- Antihistamine nasal sprays (azelastine / Astepro) — block the histamine-driven swelling response
- Saline irrigation — physically clears allergen load and improves medication penetration
- Allergen avoidance strategies — addressing the source when possible
- Immunotherapy — allergy shots or sublingual drops for appropriate candidates who want long-term desensitization
For many patients, this combination produces significant improvement — enough to restore comfortable nasal breathing without any procedure.
Step 2: Turbinate Reduction When Medical Therapy Isn't Enough
If the turbinate remains enlarged despite appropriate medical management — or if the hypertrophy has a strong structural component that sprays cannot address — we move to a turbinate reduction procedure.
Two main approaches:
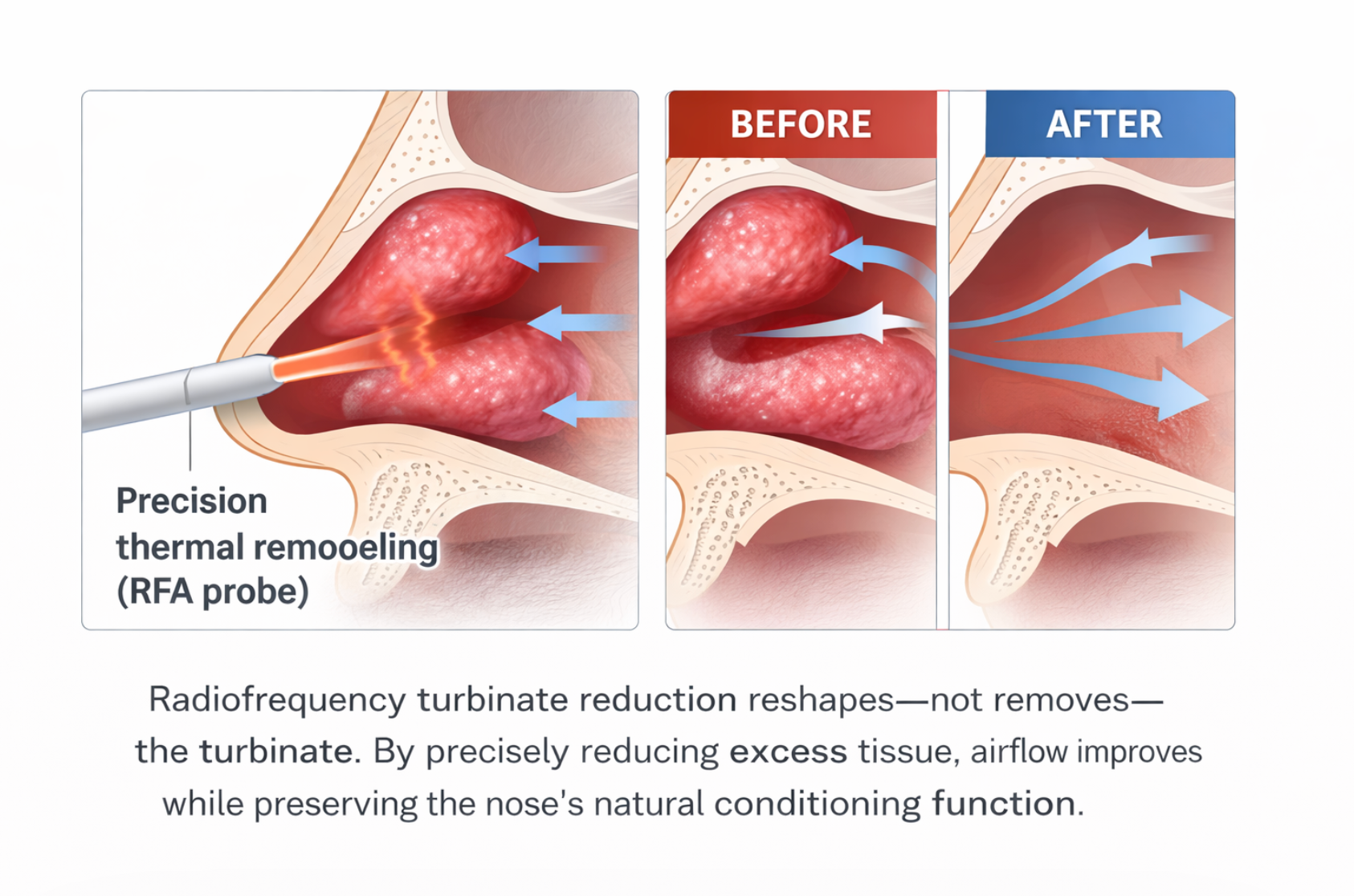
- Radiofrequency ablation (RFA): Controlled thermal energy is delivered inside the turbinate tissue using a small probe. The heat causes the tissue to contract and scar internally over the following weeks, reducing turbinate volume while keeping the outer surface intact. This is commonly done in the office under local anesthesia — no general anesthesia required, minimal downtime.
- Submucosal/microdebrider reduction: A small instrument removes tissue from inside the turbinate while preserving the mucosal surface — maintaining the turbinate's conditioning function while reducing its bulk. This is typically done in an operating room, often combined with septoplasty or sinus surgery.
⚠️ THE GOAL IS NEVER TO REMOVE THE TURBINATE — IT'S TO RIGHT-SIZE IT
A common misconception: turbinate reduction means removing the turbinate. It doesn't — and it shouldn't.
The turbinate performs critical functions: warming, filtering, and humidifying every breath. Overly aggressive turbinate removal (called 'empty nose syndrome' in its most severe form) can create a paradox where the nasal passage is physically wide open, yet the patient feels like they can't breathe — because the flow conditioning system is gone.
Good turbinate surgery is about engineering optimization, not demolition. The goal is a turbinate that takes up the right amount of space — enough to do its job, small enough to allow efficient airflow.
⚡ DRS ENABLED — THIS ISSUE'S QUICK WIN
⚡ DRS ENABLED — ONE ACTION YOU CAN TAKE TODAY
Start your nasal steroid spray correctly — and give it a real chance to work.
Flonase (fluticasone), Nasacort, and similar sprays are highly effective for allergic turbinate hypertrophy. But most patients use them wrong and quit before they work.
Here's how to do it right:
1. Tilt your head slightly forward — not back. You want the spray to land on the lateral nasal wall and turbinate, not drain down your throat.
2. Aim slightly outward (toward your ear) — not straight up toward the top of your head.
3. Use it daily for at least 2–4 weeks before deciding if it's working. These are anti-inflammatory sprays, not decongestants. They build effect over time.
4. Don't stop when you feel better — the underlying inflammation is still there. Consistency is what keeps the turbinate from swelling back.
Correct daily technique for 4 weeks will tell you far more about whether medical therapy can manage your turbinate than three days of inconsistent use.
📋 TECHNICAL REGULATIONS — THIS ISSUE'S SAFETY CHECK
📋 YOUR ALLERGY SPRAY MAY BE CAUSING YOUR NOSEBLEEDS — AND THERE’S AN EASY FIX
If you are being treated for turbinate hypertrophy or allergic rhinitis with a topical nasal steroid — such as Flonase (fluticasone) or Nasacort — or a nasal antihistamine spray such as Astepro (azelastine), and you have been experiencing nosebleeds, your spray technique is likely the culprit.
These sprays are highly effective for managing turbinate swelling and nasal allergies. But they can also dry out the nasal lining — and when the nozzle is aimed directly at the septum, the thin tissue in the middle of your nose takes the full impact of the spray with every dose. Over time, that repeated drying causes small cracks and bleeds in the septal mucosa. Epistaxis (nosebleeds) in patients on nasal sprays is one of the most common complaints I see — and it is almost always a technique problem, not a medication problem.
The Fix: Cross Your Hands When You Spray
This is a simple technique I teach every patient who uses a nasal spray, and it makes an immediate difference:
• When spraying your RIGHT nostril, hold the bottle in your LEFT hand.
• When spraying your LEFT nostril, hold the bottle in your RIGHT hand.
Crossing your hands naturally angles the nozzle away from the septum and toward the outer wall of the nasal cavity — which is exactly where you want the medication to land. The turbinate is on that outer wall. The septum gets spared.
It feels awkward the first few times. Within a week, most patients report that the nosebleeds stop entirely — without any change in medication.
The regulation: Don’t stop a medication that’s helping your turbinates because of a side effect that a simple technique fix can prevent entirely.
CLOSING — THE TAKEAWAY
CORE THESIS — ISSUE 3
Your turbinates are not the problem. They are your body's original flow-conditioning system — engineered over millions of years to warm, filter, and condition every breath you take.
When they enlarge — from allergies, medication rebound, or structural compensation — it's not a failure of design. It's a system under chronic load without the maintenance it needs.
Fix the trigger. Protect the function. Right-size the structure when needed. That's how you restore F1-grade airflow — without ripping out the very system that makes it work.
Kristina came back for a follow-up three months later. She'd been on a topical nasal steroid and antihistamine spray consistently. Her turbinates had reduced significantly — enough that she was breathing comfortably through her nose for the first time in years. We never had to do a procedure.
That's the goal. Understand the system. Manage the load. Keep the engine running the way it was designed to run.
The ENT Edge
Join Dr Gus on Substack for more actionable wellness insights and guides to help you sleep, breathe, and hear better, with spotlights on new technologies in the ear, nose and throat health category.

